A 27 year old lady, 33 weeks twin pregnancy (Full term pregnancy is between 37 and 42 weeks) had been presented in Ruby Emergency with complaints of shortness of breath for 2-3 days and had been admitted under the expert care of (Prof) Dr. Sudhir Adhikary (Consultant Obstetrics and Gynaecology). She was a known case of Hypothyroidism, Gestational Hypertension, Preeclampsia (High blood pressure and signs of organ damage, typically occurring after 20 weeks of pregnancy), Cardiomyopathy and acute decompensated heart failure as well as pedal edema (Swelling of foot or ankle). The lady was initially on Bilevel Positive Airway Pressure (BiPAP) followed by High-Flow Nasal Oxygen (HFNO). After a thorough discussion with the family members about the risk factors and with their written and informed consent she was posted for emergency caesarean section. The lady delivered live preterm twins with low birth weight, Respiratory Distress Syndrome (RDS) and Neonatal Jaundice. The lady had been intubated post surgery and was on mechanical ventilation. After gradual improvement she had been extubated.
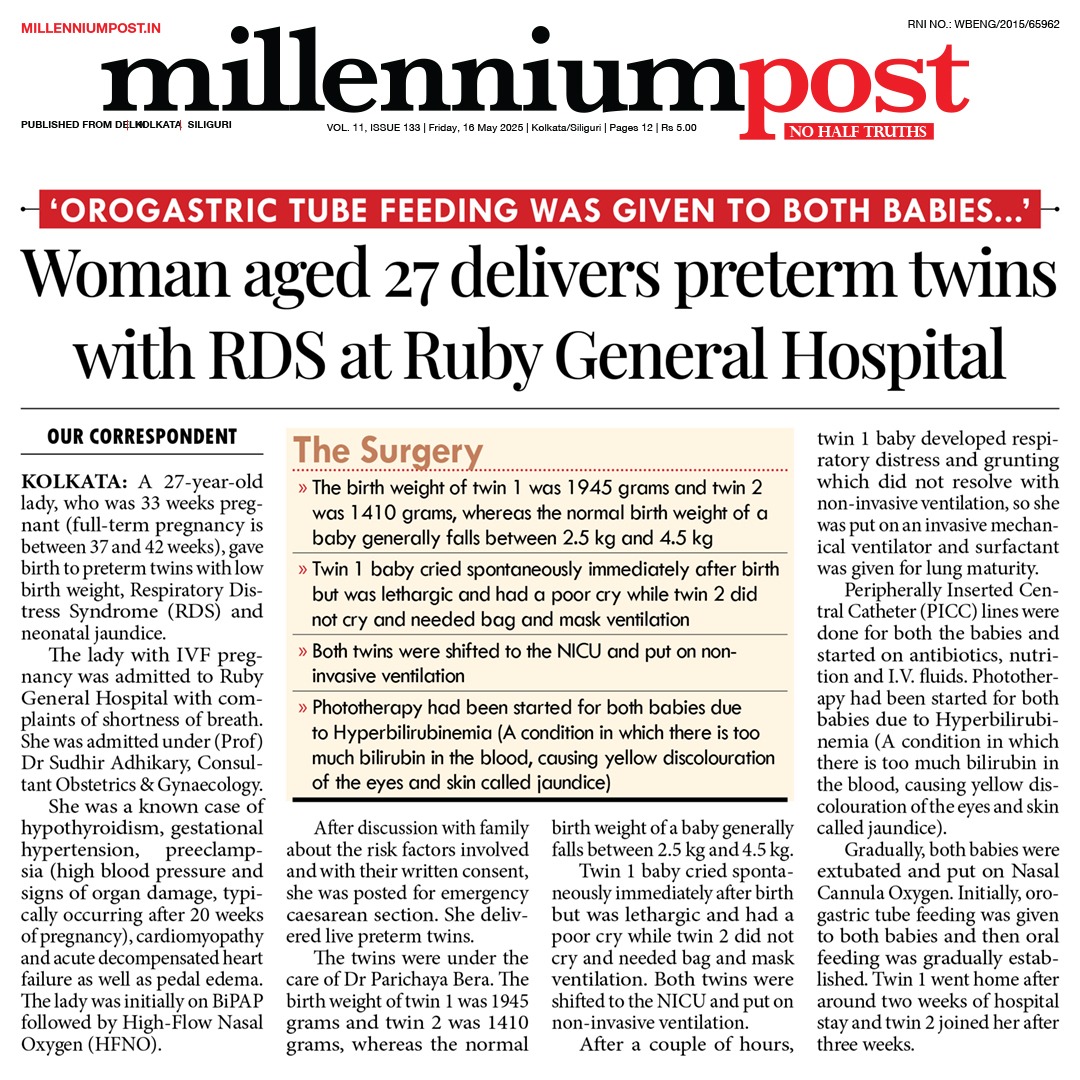
The twins had been under the care of Dr. Parichaya Bera (Consultant Paediatrician). The The birth weight of Twin 1 was 1945 grams and Twin 2 was 1410 grams whereas the normal birth weight of a baby generally falls between 2.5 kg and 4.5 kg. Twin 1 baby cried spontaneously immediately after birth but, was lethargic and had a poor cry while, Twin 2 did not cry and needed Bag and mask ventilation. Both twins were shifted to NICU and put on non invasive ventilation. After a couple of hours Twin 1 baby developed respiratory distress and grunting which did not resolve with Non invasive ventilation, so, she was put on invasive mechanical ventilator and Surfactant was given for lungs maturity. Peripherally Inserted Central Catheter (PICC) lines were done for both the babies and started on antibiotics, nutrition and I.V. fluids. Phototherapy had been started for both babies due to Hyperbilirubinemia (A condition in whch there is too much bilirubin in the blood, causing yellow discolouration of the eyes and skin called jaundice). Gradually, both the babies were extubated and put on Nasal Cannula Oxygen. Initially, orogastric tube feeding was given to both babies and then oral feeding was gradually established. Twin 1 went home after around two weeks hospital stay and Twin 2 joined her after three weeks. The parents were at a loss of words while expressing their gratitude to the expert team of Gynaecologists and Paediatricians who changed their bleak hope to a strong faith.
Gradually both the babies were shifted out from the ventilation and was put on nasal cannula oxygen. Initially orogastric tube feeding was given and then oral feeding was gradually established. Both baby needed i.v antibiotics, phototherapy, KMC and other supportive measures. The twin 1 baby was discharged around 2 weeks of hospital stay with completely stable condition and twin 2 baby was discharged around 3 weeks of hospital stay with hemodynamically stable condition.

 98311 79175
98311 79175
 ruby@rubyhospital.com
© Ruby General Hospital - 2024. All Rights Reserved. Website Managed by M9 IT Consulting Services
ruby@rubyhospital.com
© Ruby General Hospital - 2024. All Rights Reserved. Website Managed by M9 IT Consulting Services













 Whatsapp
Whatsapp


